Heart disease is the number one killer of women, and the second leading cause of death in women aged 35-64. Those frightening statistics make heart disease quite a hot topic these days. For women, heart disease is a multifactorial condition and we think it’s better to know your risks. That’s because, in many cases, you can alter your overall risk by taking action on your own.

That may sound daunting but really, it’s good news. Since information is power, you can help protect yourself well by following an approach that minimizes as many of these risk factors as possible. Understanding the progression of heart disease is a good way to start, so let’s look at its early signs and the factors that contribute to its development.
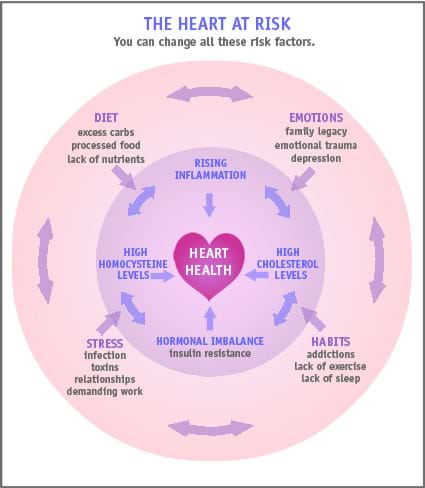
Early warning signals of heart disease: levels of cholesterol, homocysteine and inflammation
Even as our understanding grows about the causes of cardiovascular disease, one thing seems clear: it’s more than just cholesterol. We also know now that metabolism and inflammation play integral roles in the development of heart disease. And it won’t surprise you to know that other key factors include family history, age and, as we know, gender.
Cholesterol. Cholesterol is an essential fat-like substance that circulates through the blood and it’s vital for building cell walls and making hormones. Cholesterol is both consumed in food and produced by the liver, and is the foundation of hormonal and metabolic balance. Even though cholesterol is essential, there are good and bad types. If you have too much of the bad cholesterol and too little of the good kind, it’s a big risk for your cardiac health.
Lipoprotein. When we talk about cholesterol levels, we are really referring to lipoproteins or the proteins that transport and store cholesterol complexes. Low-density lipoprotein (LDL) transports cholesterol around your body and is considered the “bad” cholesterol. High levels of LDL can lead to excess cholesterol deposits on artery walls. Eventually arteries narrow, or become clogged, which reduces blood flow to the heart. That leads to heart attack or angina and/or stroke in the brain. High-density lipoprotein (HDL) — the “good” cholesterol — moves cholesterol out of the bloodstream and back to the liver where it is broken down. Total cholesterol measurement is a calculation of HDL, LDL and triglycerides. Because of this, a high cholesterol count is not necessarily bad as long as your LDL is low and HDL is high.
Recent studies have shown that the presence of certain periodontal bacteria can raise your risk of heart disease due to the inflammation they cause in the gums. These bacteria pump high levels of toxins into the blood stream where they lead to inflammation. They can then travel to other organs, including the heart and arteries, causing localized damage. For heart health and more, see your dentist at least twice a year.
Homocysteine. Homocysteine is an amino acid created in your blood when you digest protein. It’s usually converted into other, less caustic amino acids with the help of B vitamins and folic acid. If levels of vitamin B and folic acid are low, homocysteine rises, injuring the cells that line blood vessels. This damage leads to inflammation, which puts you at increased risk for clots and atherosclerosis (hardening of the arteries). Other causes of high homocysteine levels include low thyroid hormone, kidney disease, psoriasis, medications and genetic deficiencies. Consuming essential fatty acids helps reduce localized inflammation. Current research supports supplementing with omega-3 fatty acids to reduce inflammation and prevent cardiovascular disease.
Insulin resistance. When your body requires higher and higher levels of insulin for glucose metabolism, you have become insulin resistant. This state is the precursor to type II diabetes, and is commonly seen alongside obesity and high blood pressure. Evidence is mounting that sustained high insulin levels are related to chronic inflammation and subsequent cardiovascular disease. To ward off insulin resistance, eat foods with a low-to-moderate glycemic load, and maintain a healthy weight. Getting more information on insulin resistance can help you make better decisions about diet and lifestyle.
Inflammation. Chronic inflammation is a key player in the development of heart disease and has also been linked to obesity, cancer, type II diabetes, irritable bowel syndrome and Alzheimer’s disease. The mechanism that drives the effects of inflammation appears to be connected to its effects on the arteries themselves. Scientists think that inflammation destabilizes the plaques created by high levels of LDL. When pieces of plaque break off, they encourage more inflammation, and can lead to complete blockage of the arteries.

Decoding your blood test results
You may have noticed that your doctor no longer checks your cholesterol yearly. New testing guidelines deemphasize “goal” levels of LDL, and now focus on accurately assessing risk and targeting the appropriate treatment for patients at increased risk for cardiovascular disease.
Here are some common labs your doctor may order to assess your heart disease risk:
- LDL: A level of more than 130 mg/dL is considered high risk.
- HDL: A level of less than 40 mg/dL is considered high risk.
- Hs-CRP: High sensitivity C-reactive protein (CRP). Optimal level is less than 1mg/L.
- Hemoglobin A1C: This measures your average blood sugar over the course of 4-8 weeks, and is used to assess for diabetes. Optimal level is less than 5.5%. A level of 5.7-6.4% indicates you may be pre-diabetic. A level of more than 7% is diagnostic of diabetes. Women who are pre-diabetic or diabetic are at significantly increased risk of heart disease.
- Homocysteine: Optimal range is 5-8 umol/L.
Most important to your overall risk is the relationship between all of these elements. For example, if women with intermediate risk of heart disease, whether due to family history, high LDL and low HDL, or obesity, have even slightly elevated hs-CRP in their blood, they are at significantly higher risk of heart disease.
But heart disease isn’t just a matter of lab results. While these numbers are an integral part of how we assess for risk and determine the best way to prevent cardiac disease, other factors also contribute to cardiac health. This includes, believe it or not, your emotional wellbeing.
The emotional roots of heart disease
Your heart is an organ that responds to how you feel. It jumps for joy, pounds with anxiety, and breaks with sadness. Current research shows that people with heart disease are more likely to suffer from depression. We think it’s connected to certain symptoms of depression that can reduce overall physical and mental health, which increases your risk for heart disease.
Common symptoms of depression, such as loss of interest in things you used to care about, decreased energy and poor concentration can interfere with health, including compliance with medication protocols. These symptoms can also drain your motivation to care for yourself by exercising or cooking your own healthy meals. Having depression also increases your risk of death after a heart attack.
Targeting emotional health is a new experience for most conventional doctors, but more are coming around to it. New programs like the HeartMath System teach practitioners from all backgrounds how to work with patients to give them tools they can use daily to help reduce stress, channel anger constructively, and achieve emotional balance.
Your cardiovascular system may also react to unresolved emotional conflicts. Stress and emotional difficulty feed the “flight or fight” response and if it stays activated for long periods, you can have adrenal stress and fatigue, increased cholesterol levels, and a weakened immune system. All leave you prone to infection and inflammation. Because women tend to “pour their hearts out” by giving more than they receive, many of their health concerns are traced back through their emotions to a closed or exhausted heart. Woman may not become aware of this until entering menopause.

Menopause and the heart
The risk of heart disease increases greatly after menopause. The reasons are still murky, but at least part of it is likely related to estrogen deficiency that changes cardiovascular risk factors. Estrogen has been shown to have both helpful and harmful effects on your cardiovascular health. For example, studies have shown there is a small increase of LDL during the menopausal transition, and a possible decrease to the protective effect of HDL. Other possible lost cardiovascular benefits linked to a decrease in estrogen include reduced endothelial (related to the inner lining of the blood vessels) function and decreased insulin sensitivity.
High levels of estrogen have also been demonstrated to increase cardiac risk, possibly by increasing serum triglyceride levels and raising the risk of blood clots and synthesis of vascular inflammatory markers such as CRP in the liver. This is why the Women’s Health Initiative showed that both equine-based and synthetic hormone replacement therapies (e.g. Premarin) increase heart disease risk in post-menopausal women.
Hormones are a vital, complex part of your underlying physiology, so it’s highly likely that they influence all of the risk factors for heart disease. How you handle the changes during menopause will have a strong impact on your overall heart health.
Understanding the factors that affect your risk of heart disease is a good first step — but don’t stop there. The best news is that most heart disease risk factors are within your control. For more information about what you can do to protect yourself, read our article on heart disease prevention.
World Health Organization. International statistical Classification of Diseases and Related Health Problems, Tenth Revision (ICD-10). Geneva: World Health Organization, 1992. Available at https://www.who.int/classifications/icd/en/.
https://www.heart.org/HEARTORG/GettingHealthy/NutritionCenter/HealthyEating/Homocysteine-Folic-Acid-and-Cardiovascular-Disease_UCM_305997_Article.jsp
1 Bhatnagar, D., & P. Durrington. 2003. Omega-3 fatty acids: Their role in the prevention and treatment of atherosclerosis related risk factors and complications. Int. J. Clin. Pract., 57 (4), 305–314. Review.
deBree, A., et al. 2004. Evidence for a protective (synergistic?) effect of B-vitamins and omega–3 fatty acids on cardiovascular diseases. EJCN, 58 (5), 732–744. URL: https://www.nature.com/ejcn/journal/v58/n5/full/1601871a.html (accessed 12.14.2006).
Geleijnse, J., et al. 2002. Blood pressure response to fish oil supplementation: Metaregression analysis of randomized trials. J. Hypertens., 20 (8), 1493–1499.
Curtis, C., et al. 2000. n-3 Fatty acids specifically modulate catabolic factors involved in articular cartilage degradation. J. Biol. Chem. 275, 721–724.
2 Geerts, S., et al. 2002. Systemic release of endotoxins induced by gentle mastication: association with periodontitis severity. J. Periodontology, 73 (1) 73–78; URL: American Academy of Periodontology: https://www.perio.org/consumer/bacteria.htm (accessed 01.04.06).
3 Chiang, N., et al. 2005. Aspirin has a gender-dependent impact on antiinflammatory 15-epi-lipoxin A4 formation. A randomized human trial. Arterioscler. Thromb. Vasc. Biol. Nov 17; [Epub ahead of print].
Ridker, P., et al. 2005. A randomized trial of low-dose aspirin in the primary prevention of cardiovascular disease in women. NEJM, 352 (13), 1293–1304.
Further reading
Bazzano, C., et al. 2006. Effect of folic acid supplementation on risk of cardiovascular diseases. JAMA, 296 (22), 2720–2726.